6 Serious Diseases with Clinical Evidence Supporting Stem Cell Therapy, including Leukemia and Ischemic Stroke

Stem cells are unique cells that can self-renew indefinitely and differentiate into various specialized cell types. Because of these properties, stem cell therapy represents a regenerative approach that repairs and replaces damaged cells, allowing tissues and organs to regain function .[1]
Serious diseases can affect people at any age. Despite advances in modern medicine, many conditions still leave patients with long-term complications or side effects from conventional treatments, even after disease control has been achieved.
In the past, stem cell therapy was not widely used due to limitations in stem cell isolation and storage. As a result, only hematopoietic stem cells derived from bone marrow were commonly applied in clinical practice. These cells can differentiate only into red blood cells, white blood cells, and platelets, limiting their use primarily to blood-related disorders.
With advances in medical science, stem cell isolation techniques have become more effective. Mesenchymal stem cells can now be successfully isolated and stored from umbilical cord tissue and adipose tissue, while retaining their ability to self-renew and differentiate .[1] This has significantly expanded the range of medical applications for stem cell therapy.

Differences Between Stem Cell Storage Options
Stem cells can be collected from various sources, each with distinct advantages and limitations. Collecting stem cells at birth from umbilical cord blood or cord tissue involves additional storage and preservation costs, but offers important benefits compared to collection later in life:
Adult stem cell collection typically requires liposuction or bone marrow aspiration, which are invasive and potentially painful procedures. In contrast, umbilical cord tissue collection is painless and performed after birth from tissue that is normally discarded.
Umbilical cord–derived stem cells have greater proliferative and differentiation potential than adult stem cells, supporting future therapeutic possibilities .[2]
Cord-derived stem cells have not been exposed to environmental toxins, chemicals, or radiation.
Currently, numerous clinical studies have reported real-world use of mesenchymal stem cells across a wide range of diseases and age groups, primarily focusing on tissue and organ regeneration. Below are six disease examples with published clinical evidence supporting stem cell therapy.
Leukemia. Standard treatment for leukemia typically involves destroying the patient’s diseased bone marrow that produces abnormal cancerous blood cells, followed by bone marrow transplantation. However, donor–recipient incompatibility remains a common challenge in many cases.
Today, hematopoietic stem cells can be collected from umbilical cord blood at birth and preserved for future use. This approach significantly reduces the risk of immune rejection and minimizes contamination associated with donor-derived stem cells.
A study published in Pediatrics in 2007 in the United States [3] reported the case of a 3-year-old patient diagnosed with acute lymphoblastic leukemia who experienced a severe relapse after completing standard chemotherapy.
The medical team and the patient’s parents chose conventional chemotherapy combined with autologous umbilical cord blood stem cell transplantation. In this case, the parents had decided to store their child’s cord blood stem cells at birth after recognizing their potential benefits. Compared with donor stem cells, autologous stem cells reduce the risk of immune rejection and infection. The treatment was successful, and the patient remained in remission with no recurrence for 20 months following transplantation.
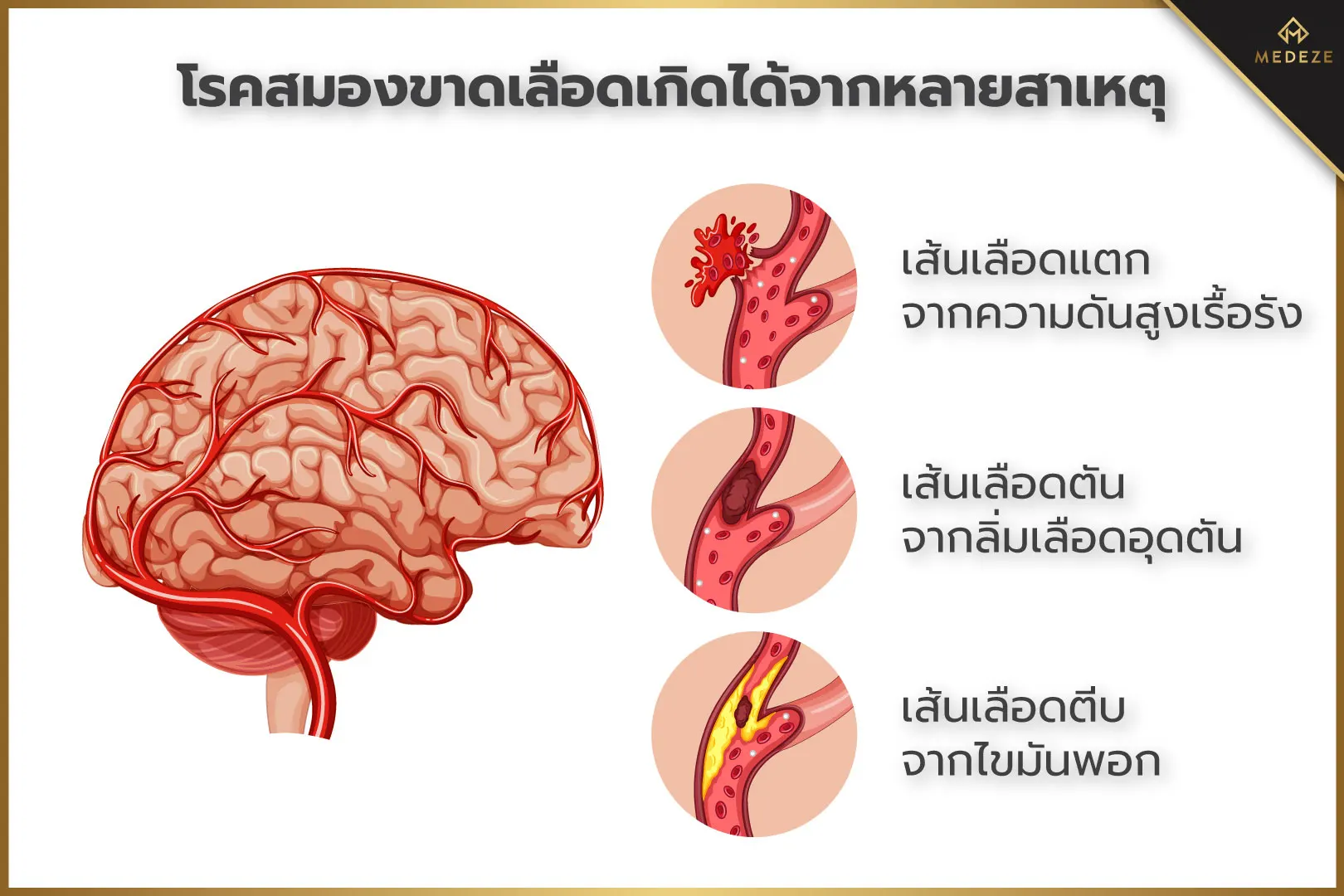
Ischemic Stroke. Ischemic stroke is associated with high mortality and long-term disability. Many patients who survive the acute phase are left with paralysis or neurological impairment. Even with intensive rehabilitation, damaged nerve cells often cannot be fully restored. Therefore, any treatment that supports neurological recovery can provide substantial benefits to both patients and their caregivers.
A long-term randomized controlled study conducted in South Korea and published in Stem Cells in 2010 [4] evaluated stem cell transplantation in patients with ischemic stroke. Participants were divided into two groups: one received intravenous autologous mesenchymal stem cells derived from their own bone marrow, while the control group did not receive stem cell therapy.
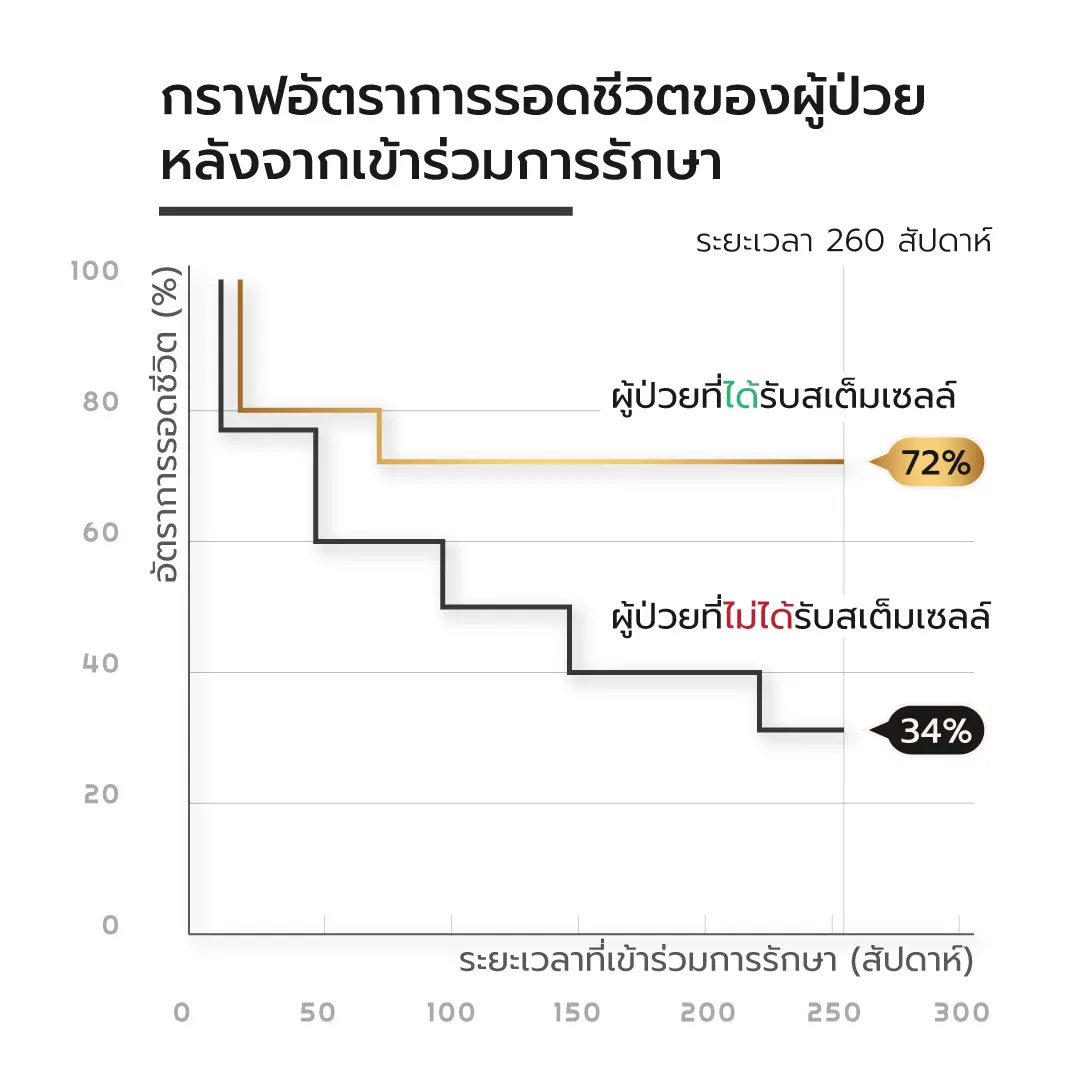
After a 5-year follow-up, the survival rate in the stem cell group was 72%, compared with 34% in the control group. In addition, patients who received stem cell therapy demonstrated greater long-term independence in daily activities. No significant differences in complication rates were observed between the two groups. These findings suggest that stem cell therapy may help reduce mortality and improve quality of life in patients with ischemic stroke.

Osteoarthritis. Regardless of the underlying cause, osteoarthritis often ultimately leads to joint replacement surgery, such as hip or knee arthroplasty. Although modern prosthetic joints can function effectively for more than 20 years, many patients are either reluctant to undergo surgery or are too young to be suitable candidates for joint replacement.
As a result, stem cell therapy has been explored as an alternative treatment for this patient group, aiming to regenerate damaged cartilage cells and slow joint degeneration. A study published in the Journal of Medical Case Reports in 2011 [3] reported outcomes in patients aged 29 and 47 with hip osteoarthritis caused by avascular necrosis, as well as patients aged 70 and 79 with knee osteoarthritis who declined joint replacement surgery.
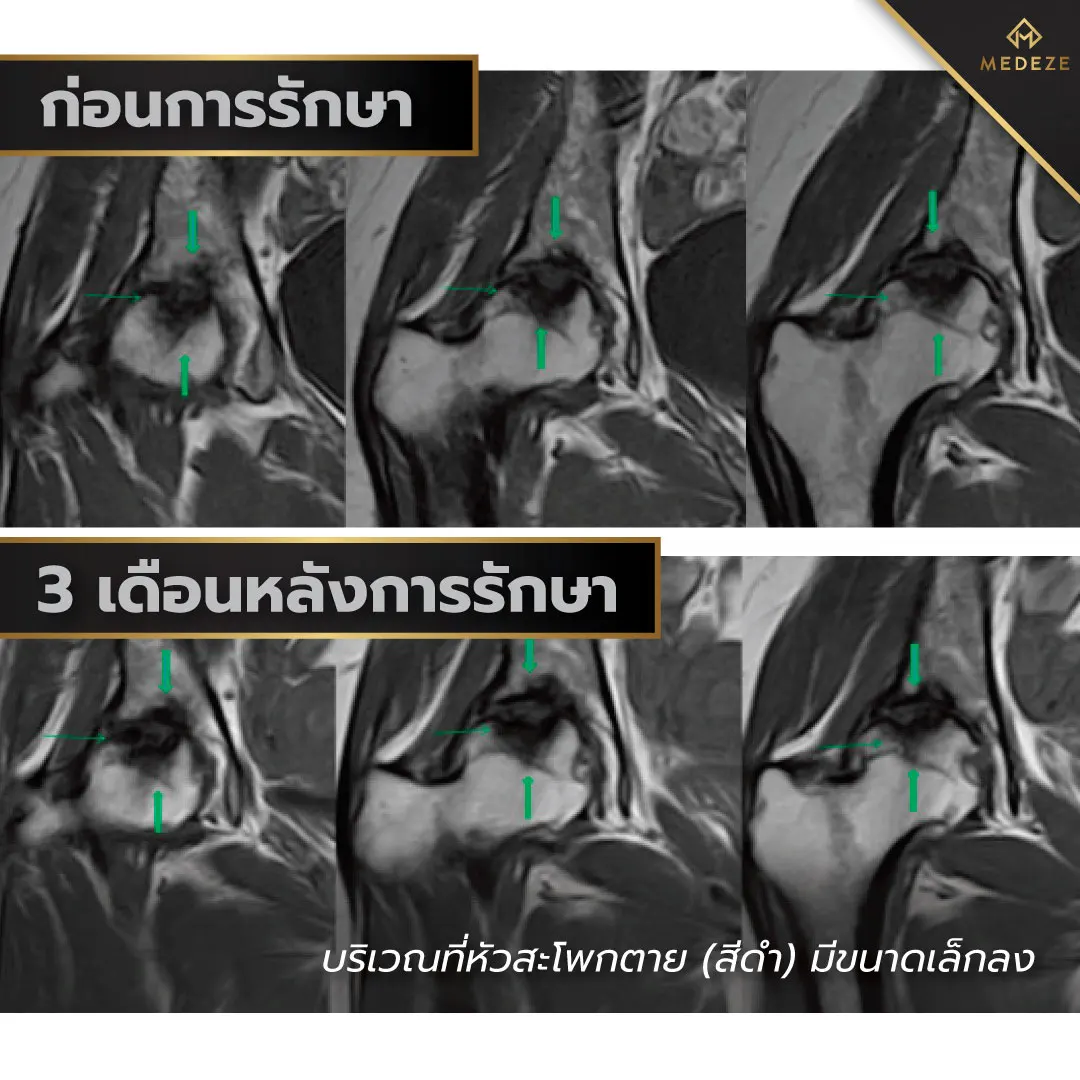
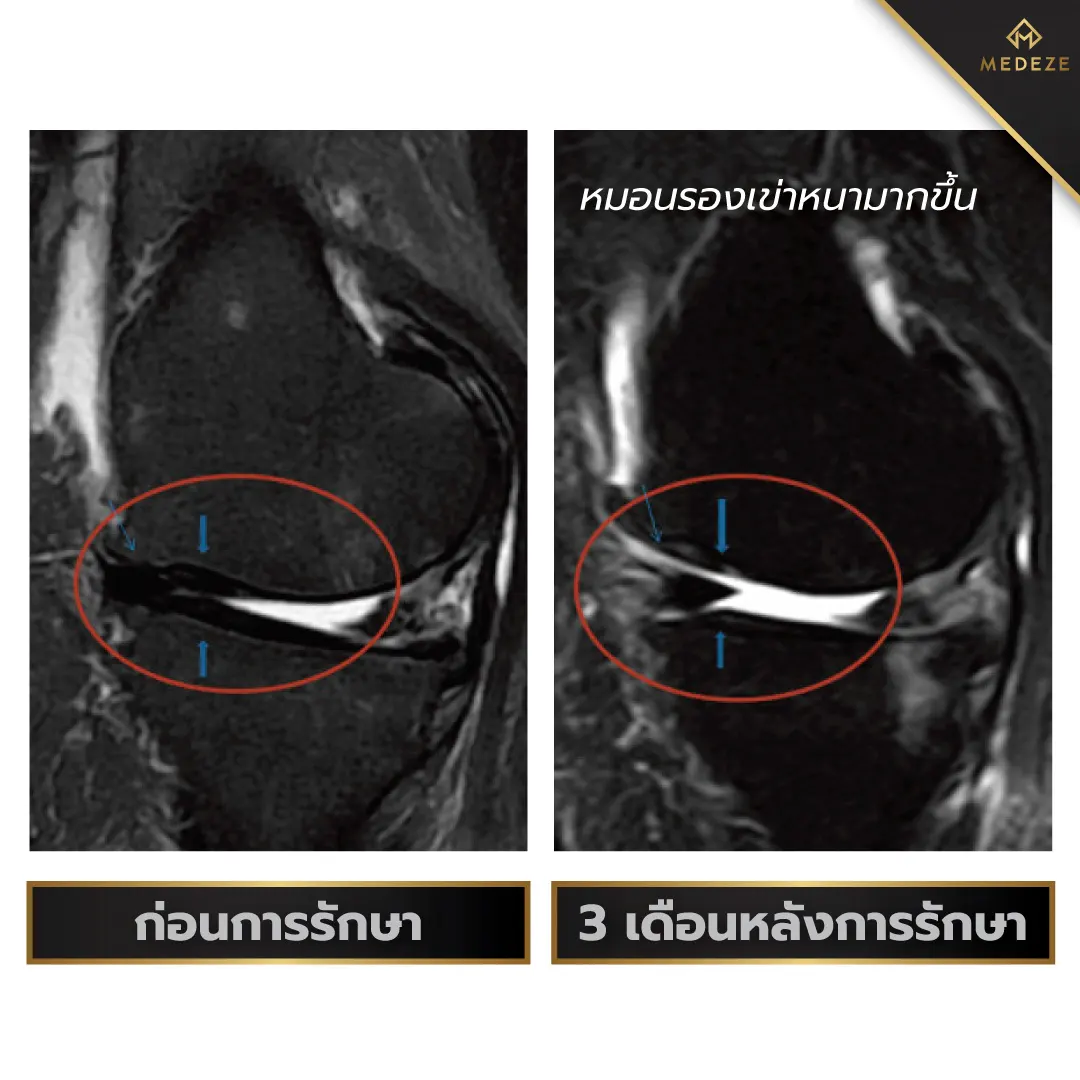
All patients received intra-articular injections of autologous adipose-derived stem cells combined with viscosupplementation. MRI evaluations performed before and after treatment demonstrated new bone and cartilage formation in all four patients. In addition, patients experienced reduced pain and improved joint mobility compared with pre-treatment assessments. These findings suggest that stem cell therapy offers a promising regenerative approach for osteoarthritis and may be extended to the treatment of degenerative joint disease in other anatomical locations.
Diabates. Type 2 diabetes is a common disease resulting from abnormal glucose metabolism, leading to elevated blood glucose levels. Standard treatment strategies begin with weight reduction, dietary control, and glucose-lowering medications. However, many patients eventually require supplementary insulin injections.
A study from China, published in Frontiers of Medicine in 2011 ,[6] investigated the use of stem cells derived from placental tissue in 10 patients with type 2 diabetes mellitus. The stem cells were administered intravenously on three occasions. The results showed that the average daily insulin requirement decreased from 63.7 to 34.6 units, with no serious adverse effects reported. These findings offer hope for improving the quality of life of patients with diabetes who depend on insulin therapy.

Subsequently, additional studies on diabetic patients have continued to be published. For example, a controlled study conducted in India and published in Cell Transplant in 2014 [7] reported similar outcomes. The study found that patients who received stem cell therapy reduced their insulin use by 66.7%, compared with only 32.1% in the control group. In this study, stem cells were derived from the patients’ own bone marrow.

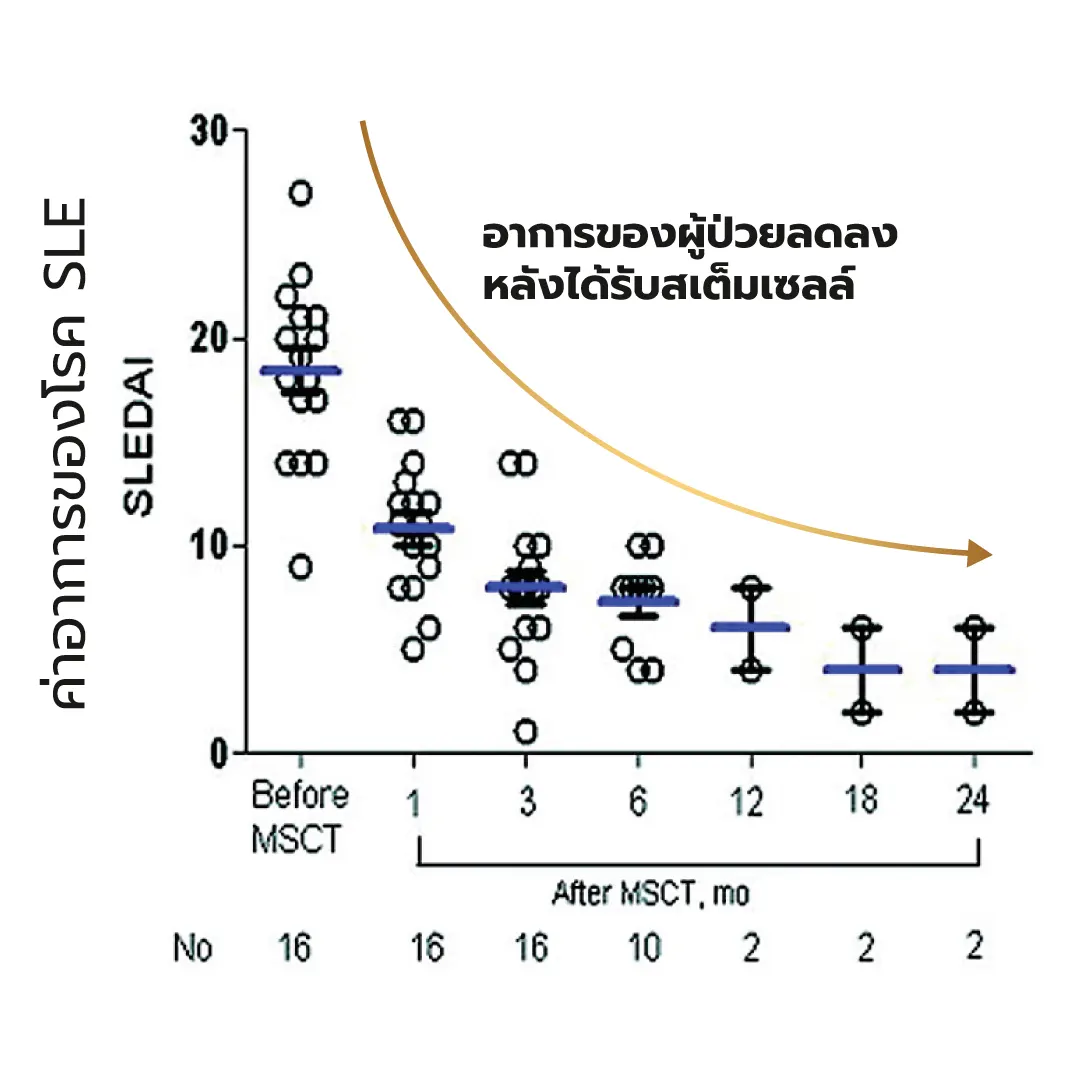
Systemic lupus erythematosus. Systemic lupus erythematosus (SLE), commonly known as lupus, is an autoimmune disease caused by dysfunction of the immune system, leading to immune-mediated attacks against the body’s own tissues and resulting in multi-organ damage. Current treatment relies primarily on immunosuppressive medications to control disease activity. However, long-term use of immunosuppressive drugs is frequently associated with significant adverse effects.
Stem cell therapy has been explored as an alternative treatment approach, based on evidence suggesting that mesenchymal stem cells can replace dysfunctional bone marrow cells in affected patients. A study from China, published in Arthritis & Rheumatism in 2010 ,[8] investigated patients with severe and refractory systemic lupus erythematosus who did not respond to conventional immunosuppressive therapy. Patients received intravenous infusions of donor-derived umbilical cord mesenchymal stem cells. At the 8-month follow-up, patients demonstrated significant overall clinical improvement, including marked reductions in inflammatory markers and substantial improvement in renal function. Notably, even after discontinuation of treatment, all patients maintained good disease control.

End-stage liver cirrhosis. For patients with end-stage liver cirrhosis, liver transplantation combined with long-term immunosuppressive therapy is the final therapeutic option. However, transplantation requires waiting for a suitable donor, which may take a prolonged period and, in some cases, leads to disease progression and clinical deterioration.
Stem cell therapy is an alternative approach aimed at restoring hepatic function. A study from Sweden, published in the European Journal of Gastroenterology & Hepatology in 2009, investigated the intravenous administration of autologous bone marrow–derived stem cells [9] in patients with end-stage liver cirrhosis. All eight participants in the study had advanced cirrhosis. Following treatment, significant improvements were observed in liver function parameters, coagulation profiles, and markers of hepatic metabolic waste compared with baseline values, without any reported complications.[8]
From the perspective of patients with end-stage liver disease, the use of autologous stem cells (Collected and preserved while the patient is still in good health) offers advantages over donor-derived stem cells. This approach reduces the risk of immune rejection and may also be beneficial in the event of future liver transplantation.

References
1) Nair V, Talwar P, Kumar S, Chatterjee T. Umbilical cord blood transplantation and banking. Pregnancy medicine. 1st ed. Delhi: Jaypee Brothers Medical Publishers (P) Ltd. 2015:197-215.
2) Mayani H. Biological differences between neonatal and adult human hematopoietic stem/progenitor cells. Stem cells and development. 2010 Mar 1;19(3):285-98.
3) Hayani A, Lampeter E, Viswanatha D, Morgan D, Salvi SN. First report of autologous cord blood transplantation in the treatment of a child with leukemia. Pediatrics. 2007 Jan 1;119(1):e296-300.
4) Lee, J. S., Hong, J. M., Moon, G. J., Lee, P. H., Ahn, Y. H., & Bang, O. Y. (2010). A long‐term follow‐up study of intravenous autologous mesenchymal stem cell transplantation in patients with ischemic stroke. Stem cells, 28(6), 1099-1106.
5) Pak, J. (2011). Regeneration of human bones in hip osteonecrosis and human cartilage in knee osteoarthritis with autologous adipose-tissue-derived stem cells: a case series. Journal of medical case reports, 5(1), 1-8.
6) Jiang, R., Han, Z., Zhuo, G., Qu, X., Li, X., Wang, X., ... & Han, Z. C. (2011). Transplantation of placenta-derived mesenchymal stem cells in type 2 diabetes: a pilot study. Frontiers of medicine, 5(1), 94-100.
8) Sun, L., Wang, D., Liang, J., Zhang, H., Feng, X., Wang, H., ... & Shi, S. (2010). Umbilical cord mesenchymal stem cell transplantation in severe and refractory systemic lupus erythematosus. Arthritis & Rheumatism, 62(8), 2467-2475.
9) Kharaziha, P., Hellström, P. M., Noorinayer, B., Farzaneh, F., Aghajani, K., Jafari, F., ... & Soleimani, M. (2009). Improvement of liver function in liver cirrhosis patients after autologous mesenchymal stem cell injection: a phase I–II clinical trial. European journal of gastroenterology & hepatology, 21(10), 1199-1205.